
Why Your Plantar Fasciitis Keeps Coming Back — And What Actually Fixes It
You felt it first on a Tuesday morning — that sharp, stabbing pain in your heel the moment your foot hit the floor. You've heard it before, maybe from a friend, a coach, or a quick Google search: plantar fasciitis. The advice that followed probably included rest, stretching, a new pair of shoes, maybe a night splint.
And yet here you are, still dealing with it.
Plantar fasciitis is one of the most common musculoskeletal complaints in active adults — affecting roughly 2 million people annually in the United States alone. It's also one of the most commonly mismanaged. The standard advice fails a significant portion of patients not because they didn't follow it, but because it doesn't address what's actually driving the problem.
What follows is the evidence-based version of this conversation — what plantar fasciitis actually is, what's really causing it, what doesn't work and why, and what a comprehensive, clinician-led approach looks like when it's done correctly.
1. What Plantar Fasciitis Actually Is — And Isn't
The name itself is misleading. The suffix "-itis" implies inflammation, but a landmark 2003 histological study by Lemont et al. published in the Journal of the American Podiatric Medical Association examined plantar fascia tissue from surgical specimens and found no inflammatory cells. What they found instead was myxoid degeneration, collagen necrosis, and angiofibroblastic changes — hallmarks of a degenerative process, not an acute inflammatory one.
This matters clinically because treatments designed to reduce inflammation — cortisone injections, NSAIDs, rest — are targeting a mechanism that isn't driving the pathology in most chronic cases. The correct term is plantar fasciosis: a failed healing response in the connective tissue of the plantar fascia, similar in nature to the degenerative tendinopathies seen at the Achilles or patellar tendon.
Plantar fasciitis is not an inflammation problem. It's a load tolerance problem — your plantar fascia is being asked to handle more stress than it currently has the capacity to absorb. The solution is building that capacity, not avoiding load.
2. The Root Causes Most Clinicians Miss
A 2003 case-control study by Riddle et al. published in the Journal of Bone and Joint Surgery remains one of the most cited investigations into plantar fasciitis risk factors. Their findings were striking: limited ankle dorsiflexion carried an odds ratio of 23.3 — meaning individuals with restricted ankle mobility were over 23 times more likely to develop plantar fasciitis than those with adequate range of motion.
Read that again. Not tight calves. Not bad shoes. Not high arches. Limited ankle dorsiflexion — the ability to bring your shin toward your foot — was the single strongest modifiable predictor of plantar fasciitis in that study.
This makes mechanical sense. When the ankle can't dorsiflex adequately during walking, running, or squatting, the foot compensates — often through excessive pronation, early heel rise, or altered loading patterns that concentrate repetitive stress at the plantar fascia insertion. The fascia isn't failing randomly. It's failing because the system upstream of it is restricted.
Additional well-documented risk factors include:
Weakness of the foot intrinsic muscles and the calf complex — the dynamic stabilizers that absorb load before the plantar fascia has to
Hip abductor and external rotator weakness — altering lower extremity alignment under load
Reduced single-leg functional strength and stability
Training load spikes — increasing mileage, volume, or intensity faster than tissue can adapt
Prolonged time on feet on hard surfaces without adequate load management
Wearing et al.'s 2006 review in Sports Medicine reinforced the kinetic chain perspective, noting that plantar fascia loading is directly influenced by rearfoot mechanics, ankle joint mobility, and Achilles tendon flexibility — all structures proximal to the foot itself. Treating the heel in isolation while ignoring the chain above it is why so many cases don't resolve.
3. What the Evidence Says About Common Treatments
Most people arrive at physical therapy having already tried some combination of the following. Here's what the research actually says:
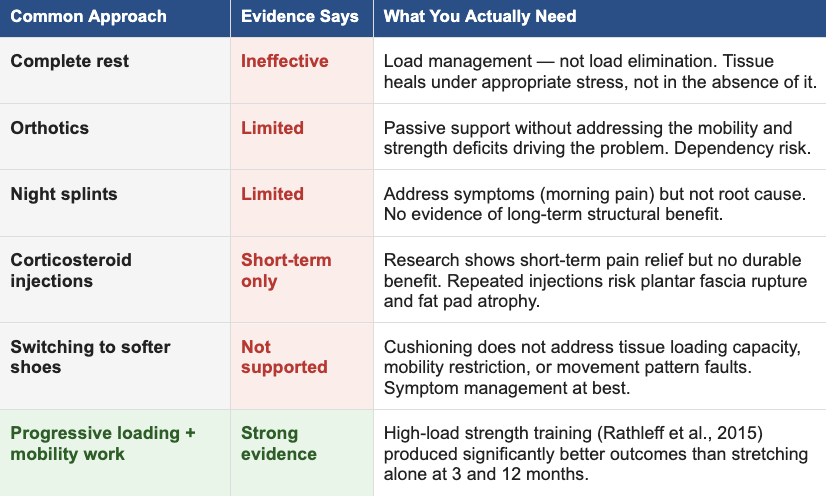
The corticosteroid data deserves particular attention. A systematic review by Coombes et al. (2010) published in The Lancet examining corticosteroid injections across musculoskeletal conditions found that while injections produced superior short-term pain relief, they were associated with worse outcomes at intermediate and long-term follow-up compared to placebo. For the plantar fascia specifically, repeated injections carry documented risk of fat pad atrophy and fascia rupture — a meaningful complication in an already compromised structure.
The message isn't that these interventions have no place. It's that they are incomplete answers to a mechanical problem — and using them as primary treatment delays the interventions that actually produce durable resolution.
4. What the Evidence Says Works — And How We Apply It
The most important shift in plantar fasciitis management over the last decade has been the move from passive, load-avoiding treatments toward active, progressive tissue loading. The landmark evidence came from Rathleff et al.'s 2015 randomized controlled trial in the Scandinavian Journal of Medicine & Science in Sports, which compared high-load strength training (heavy slow resistance calf raises on a step) against standard plantar fascia stretching.
At 3 months, the high-load group showed significantly greater improvements in pain and function. At 12 months, the high-load group maintained superior outcomes. This wasn't a marginal difference — it fundamentally reframed how evidence-based clinicians approach this condition. The plantar fascia responds to progressive mechanical loading the same way a tendon does: load it appropriately, and it adapts and strengthens. Protect it indefinitely, and it doesn't.
The goal of treatment is not to protect the plantar fascia from stress. It's to systematically increase the plantar fascia's capacity to tolerate stress — while simultaneously addressing every upstream factor that was overloading it in the first place.
At Ascent Total Performance, that means a comprehensive approach that goes well beyond the foot
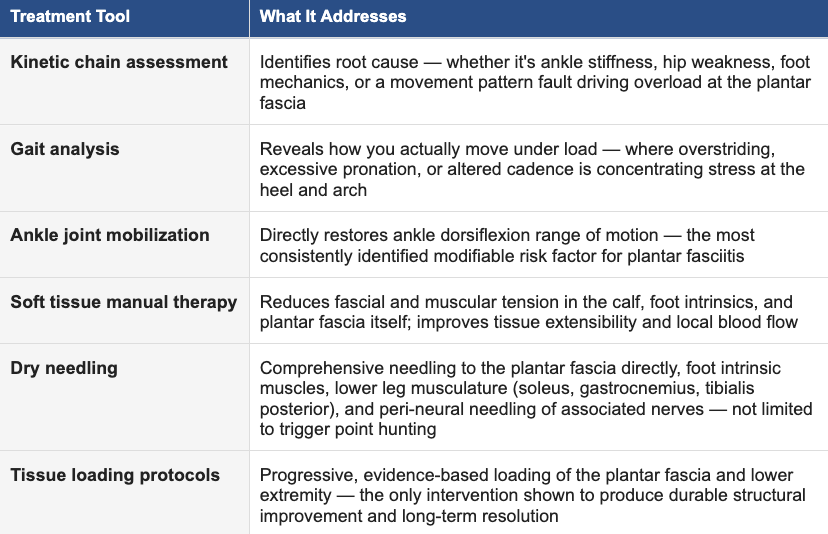
The kinetic chain assessment is where this starts — and it's what separates a thorough clinical evaluation from a generic protocol. We are looking at how you move, where your system is restricted or weak, and what's driving excessive demand on the plantar fascia. Ankle dorsiflexion is measured. Hip strength is assessed. Your gait is analyzed under load. The plan that comes out of that evaluation is specific to your body — not a standardized handout.
Our dry needling approach to plantar fasciitis goes well beyond trigger point work. We needle the plantar fascia directly to drive a local tissue healing response, address the intrinsic muscles of the foot and the full lower leg musculature — including the soleus, gastrocnemius, and tibialis posterior — and use peri-neural needling to target the associated nerves contributing to pain sensitization. This is a comprehensive, structure-specific approach that treats the entire tissue environment, not just the most symptomatic spot. Joint mobilization of the ankle, subtalar, and midfoot joints restores the range of motion that passive stretching alone rarely achieves. And the loading protocols we prescribe are progressive and challenging — because under-dosing the tissue is one of the most common reasons loading programs fail.
5. You Don't Have to Stop Training
This is the conversation most active people need but rarely get. The default advice — rest until it feels better — sets up a cycle that many athletes know too well: rest, feel better, return to activity, pain comes back. That's not recovery. That's management of a problem that was never actually addressed.
For the vast majority of our patients, the goal is to keep you moving — with intelligent load modification in the short term while we build the tissue capacity and correct the mechanical factors that got you here. That might mean adjusting your training volume temporarily, modifying the surfaces you train on, or changing the sequencing of your workouts. It rarely means stopping entirely.
DiGiovanni et al. (2003, Journal of Bone and Joint Surgery) demonstrated that exercise-based interventions outperformed passive approaches in both pain reduction and functional improvement — and that active patients who maintained modified training throughout treatment had better long-term outcomes than those who stopped completely.
We are experienced at navigating this with athletes and active adults. The goal is always a quick, complete return to full activity — not just making the pain manageable enough to function.
6. What to Expect When You Work With Us
Your first visit starts with a comprehensive assessment — not just of your foot, but of your entire lower extremity kinetic chain. We want to understand the full picture before we prescribe anything.
From there, treatment is built around your specific findings, your goals, and how long you've been dealing with this. For some patients, particularly those who come in early, we can produce significant, meaningful symptom improvement within the first one to two visits. Others with longer symptom histories or more complex presentations may work with us over a period of weeks — typical timelines range from a handful of sessions to around 12 weeks for more chronic cases. There is no fixed protocol because there is no fixed patient.
What we can tell you is that our outcomes consistently outperform the standard of care for this condition. That's not a claim we make lightly — it's the result of treating the whole system rather than just the symptom, applying hands-on interventions that most clinics don't offer, and prescribing loading protocols that are actually challenging enough to drive adaptation. The goal is never to manage your plantar fasciitis indefinitely. It's to resolve it.
The Bottom Line
Plantar fasciitis is not a life sentence, and it's not a reason to stop doing what you love. It is a signal that your system has a deficit — in mobility, in strength, in load tolerance — that needs to be addressed directly. The sooner you get a thorough evaluation and start building in the right direction, the faster and more completely you recover.
No referral needed. If your heel has been limiting you, let's take a complete look at what's driving it and build a plan to get you back.
Disclaimer: This content is for educational purposes only and does not constitute medical advice. Always consult with your physician or a licensed physical therapist before beginning any new exercise or rehabilitation program.
📅 Ready to actually fix it? Request an appointment at achieveatp.com — no referral required.
REFERENCES
All studies peer-reviewed and indexed. Verify at pubmed.ncbi.nlm.nih.gov.
Lemont H, Ammirati KM, Usen N. (2003). Plantar fasciitis: a degenerative process (fasciosis) without inflammation. Journal of the American Podiatric Medical Association, 93(3), 234–237.
Riddle DL, Pulisic M, Pidcoe P, Johnson RE. (2003). Risk factors for plantar fasciitis: a matched case-control study. Journal of Bone and Joint Surgery, 85(5), 872–877.
Rathleff MS, Mølgaard CM, Fredberg U, et al. (2015). High-load strength training improves outcome in patients with plantar fasciitis: a randomized controlled trial with 12-month follow-up. Scandinavian Journal of Medicine & Science in Sports, 25(3), e292–300.
DiGiovanni BF, Nawoczenski DA, Lintal ME, et al. (2003). Tissue-specific plantar fascia-stretching exercise enhances outcomes in patients with chronic heel pain. Journal of Bone and Joint Surgery, 85(7), 1270–1277.
Wearing SC, Smeathers JE, Urry SR, Hennig EM, Hills AP. (2006). The pathomechanics of plantar fasciitis. Sports Medicine, 36(7), 585–611.
Coombes BK, Bisset L, Vicenzino B. (2010). Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. The Lancet, 376(9754), 1751–1767.
Buchbinder R. (2004). Plantar fasciitis. New England Journal of Medicine, 350(21), 2159–2166.
Martin RL, Davenport TE, Reischl SF, et al. (2014). Heel pain — plantar fasciitis: revision 2014. Clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the APTA. Journal of Orthopaedic & Sports Physical Therapy, 44(11), A1–A33.
Cheung JT, Zhang M, An KN. (2006). Effect of Achilles tendon loading on plantar fascia tension in the standing foot. Clinical Biomechanics, 21(2), 194–203.
Trojian T, Tucker AK. (2019). Plantar fasciitis. American Family Physician, 99(12), 744–750.