
Creatine: What the Science Actually Says
Creatine has an image problem. To most people, it's the supplement in the giant tub at GNC that football players use to get bigger. It's associated with bulking, water retention, and maybe some vague concern about your kidneys.
That image is wrong — and it's costing a lot of people real results they could be getting.
With over 500 peer-reviewed studies behind it, creatine monohydrate is the most researched ergogenic supplement in the history of sports science. The evidence covers strength and muscle, yes — but also brain performance, cognitive resilience, longevity, and healthy aging. And the dosing conversation has quietly evolved in ways that most people — and most clinicians — haven't caught up with yet.
Here's what the science actually says.
1. What Is Creatine — And What Does It Actually Do?
Creatine is a naturally occurring compound synthesized in your liver and kidneys from three amino acids: arginine, glycine, and methionine. You also consume it through meat and fish. Your body stores approximately 95% of it in skeletal muscle as phosphocreatine (PCr), with the remaining 5% distributed in the brain, heart, and other metabolically active tissues.
Think of phosphocreatine as a fast-access battery backup. During high-intensity activity — a heavy set, a sprint, a cognitive sprint — your primary energy currency (ATP) depletes rapidly. Phosphocreatine steps in as the immediate phosphate donor to rapidly regenerate ATP, extending your capacity before fatigue sets in.
Supplemental creatine expands this phosphocreatine reservoir by 10–40% above dietary baseline. More stored creatine means a larger battery, a faster recharge between efforts, and — as we'll cover — a meaningfully different brain when dosing is high enough to penetrate the blood-brain barrier.
Creatine doesn't make you perform better by magic. It gives your body more of the raw material it uses to sustain high-intensity effort — physical or cognitive. The effort still has to be there.
2. Strength & Muscle: The Foundation
This is where creatine's reputation was built — and the evidence is overwhelming. Across hundreds of controlled trials and multiple large meta-analyses, creatine monohydrate consistently produces meaningful improvements in maximal strength, power output, lean mass, and muscular endurance when combined with progressive resistance training.
Rawson & Volek's landmark 2003 meta-analysis of 22 randomized controlled trials found creatine produced ~8% greater maximal strength gains compared to placebo. A 2017 meta-analysis by Lanhers et al. confirmed significant improvements in both upper and lower limb strength, with the strongest effects in higher-volume training protocols.
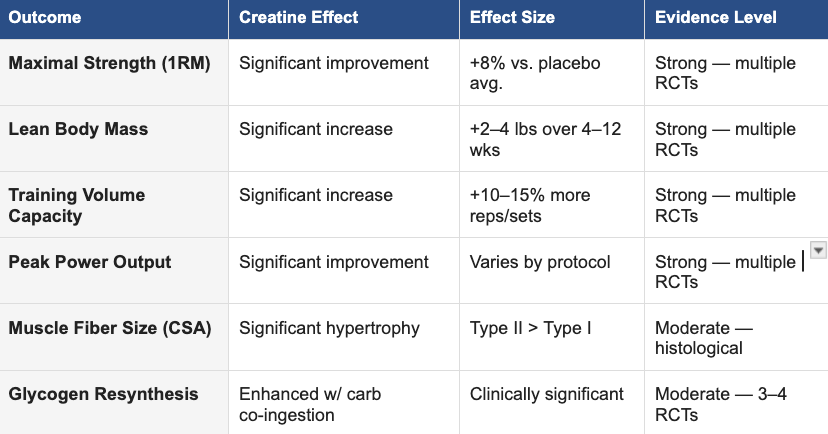
Why does it work so well? Three primary mechanisms: First, creatine allows more total work per session by sustaining energy availability through hard sets — and total training volume is the primary mechanical driver of hypertrophy. Second, research shows creatine upregulates myogenic regulatory factors (including MyoD and myogenin) that promote satellite cell activity and muscle fiber development — a distinct anabolic pathway beyond just energy availability. Third, when taken with carbohydrates post-workout, creatine significantly enhances muscle glycogen replenishment via GLUT-4 upregulation, improving recovery quality and subsequent training readiness.
3. Brain Performance: The Benefit Most People Don't Know About
Your brain consumes approximately 20% of your total body energy while accounting for only 2% of your body mass. It runs on the same phosphocreatine energy system as your muscles — and it's equally vulnerable to creatine depletion under stress.
When brain creatine is low, working memory degrades, processing speed slows, and executive function suffers — particularly under conditions of sleep deprivation, hypoxia, or sustained cognitive demand. Supplemental creatine can directly address this.
A 2003 double-blind crossover trial by Rae et al. (Proceedings of the Royal Society B) found that creatine supplementation in vegetarians — who have lower dietary creatine intake and thus lower brain creatine baseline — produced significant improvements in working memory and intelligence test scores. Avgerinos et al.'s 2018 systematic review and meta-analysis confirmed that creatine significantly improves short-term memory and reasoning, with the largest effects in older adults and those under physiological stress.
Perhaps the most clinically striking study: McMorris et al. (2007) administered creatine during 24 hours of sleep deprivation and found the creatine group significantly outperformed placebo on complex cognitive tasks — randomized number generation, backward digit span, and choice reaction time. The cognitive impairment associated with sleep loss was measurably blunted.
The catch: standard doses of 3–5 g/day are likely insufficient to meaningfully raise brain creatine levels. The brain is protected by a transport-limited blood-brain barrier — you need elevated plasma concentrations, achieved with 10–20 g/day, to drive meaningful CNS uptake.
Who benefits most from the cognitive angle: people managing high mental workloads or long hours, anyone dealing with inconsistent sleep, vegetarians and vegans (lower dietary baseline), adults 40+ (brain creatine declines with age), and athletes in high-volume training blocks where physical stress taxes mental sharpness.
4. Aging & Longevity: A Tool Most 45+ Adults Are Underusing
After age 30, skeletal muscle mass declines at 1–2% per year. After 60, that rate accelerates. This process — sarcopenia — is one of the most significant contributors to reduced quality of life, metabolic decline, fall risk, and loss of independence in older adults. Creatine, combined with resistance training, is among the most evidence-backed tools available to slow it.
Dr. Darren Candow, whose body of work represents the most comprehensive investigation of creatine and aging, has demonstrated that older adults require 0.1–0.3 g/kg/day — roughly 7–21 g for most adults — combined with resistance training to achieve meaningful lean mass preservation, functional strength gains, and bone density protection. His 2019 review in the Journal of the International Society of Sports Nutrition explicitly noted that standard 3–5 g/day doses frequently fail to reach statistical or clinical significance in this population.
Forbes & Candow's 2021 synthesis concluded that higher doses with progressive resistance training represent a safe and clinically viable strategy to attenuate sarcopenia, improve functional outcomes — grip strength, gait speed, chair-stand performance — and support long-term quality of life.
If you're over 45 and taking only 3–5 g/day, you're likely leaving the most meaningful benefit on the table. The evidence supports 10 g/day as the floor for this population — paired with consistent resistance training.
5. How Much Should You Take? A Goal-Based Guide
There is no single correct dose — the right amount depends on your goals, your baseline, and your biology. Vegetarians, vegans, older adults, and anyone under high physiological or cognitive stress tend to have lower creatine stores and exhibit a greater response to supplementation. Here's a practical breakdown:
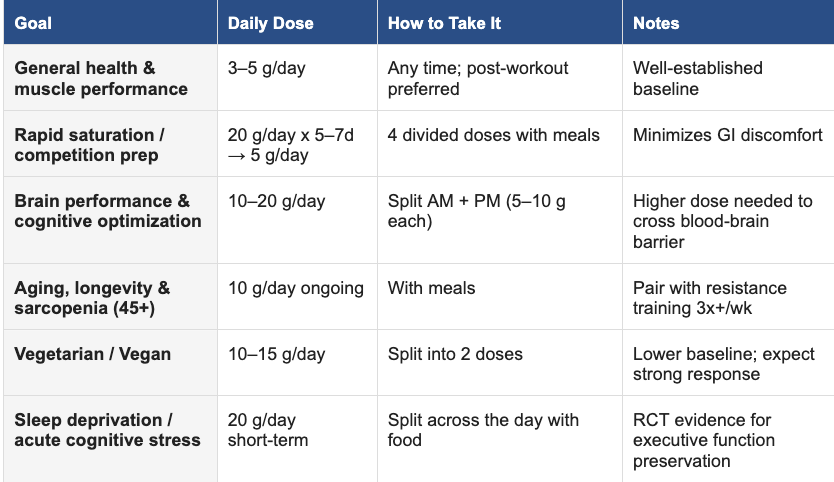
A note on loading: the classic 20 g/day for 5–7 days protocol saturates muscle phosphocreatine approximately 20% faster than lower chronic dosing (Hultman et al., 1996, Journal of Applied Physiology). It's useful for rapid saturation in time-sensitive performance contexts. For cognitive and longevity goals, sustained higher dosing without a formal loading phase is equally effective and easier to manage.
6. What Form to Buy — And What to Avoid
Creatine monohydrate. That's it. Despite aggressive supplement marketing for creatine HCl, ethyl ester, buffered creatine, and various proprietary blends, no alternative form has outperformed plain creatine monohydrate in a legitimate head-to-head trial. And monohydrate is a fraction of the cost.
Look for: Creapure-certified creatine monohydrate (manufactured in Germany to pharmaceutical-grade purity standards)
Look for: NSF Certified for Sport or Informed Sport label if you're a competitive athlete subject to drug testing
Avoid: Proprietary blends that obscure the actual creatine dose
Avoid: Brands with no third-party testing verification
7. Side Effects: What's Real, What's a Myth, What's Worth Knowing
Creatine has an exceptional safety record. The ISSN position stand (Kreider et al., 2017) confirms that doses of 3–30 g/day are safe for up to 5 years in healthy individuals — a conclusion supported by one of the largest bodies of safety data in all of sports nutrition. Here's the honest breakdown:
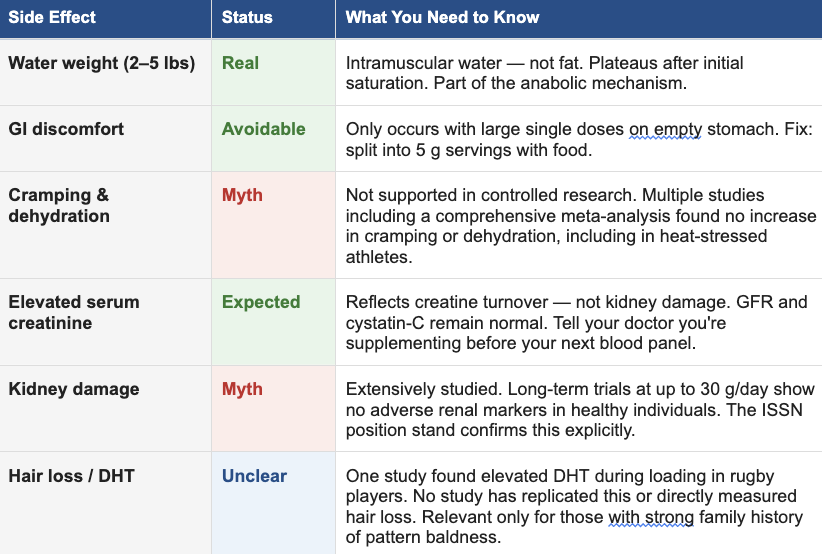
One important practical note: creatine supplementation raises serum creatinine on standard blood panels. This is expected and benign — it reflects increased creatine turnover, not kidney stress. GFR and cystatin-C remain the clinically valid markers. Always disclose supplementation status to your physician before labs.
Who should consult their physician first: anyone with chronic kidney disease (stage 3+), polycystic anyone with a diagnosed creatine metabolism disorder.
The Bottom Line
Creatine monohydrate is not a shortcut. It's a well-researched tool that extends what your training, your brain, and your biology can do — when used correctly, at the right dose for your goals. The evidence is stronger, broader, and more nuanced than most people realize. And the dosing conversation has moved beyond the 5 g/day default that most people are stuck on.
Whether you're chasing strength, trying to maintain your edge at 50, managing a demanding cognitive workload, or recovering from an injury — there's likely a version of this that serves you. Supplementation is most effective when it's personalized. If you want a recommendation tailored to your specific goals and baseline, bring it up at your next visit or reach out directly.
Want a supplementation approach built around your goals? Talk to us at your next visit or reach out at achieveatp.com.
Disclaimer: This content is for educational purposes only and does not constitute medical advice. Always consult with your physician before beginning any supplement or exercise routine, particularly if you have a pre-existing health condition or are taking prescription medications.kidney disease, those on nephrotoxic medications, individuals who are pregnant or breastfeeding, or
REFERENCES
All studies peer-reviewed and indexed. Verify at pubmed.ncbi.nlm.nih.gov.
Rawson ES, Volek JS. (2003). Effects of creatine supplementation and resistance training on muscle strength and weightlifting performance. Journal of Strength and Conditioning Research, 17(4), 822–831.
Lanhers C, et al. (2017). Creatine supplementation and upper limb strength performance: A systematic review and meta-analysis. European Journal of Sport Science, 17(7), 928–937.
Volek JS, et al. (2004). The effects of creatine supplementation on muscular performance and body composition responses to short-term resistance training overreaching. European Journal of Applied Physiology, 91(5–6), 628–637.
Rae C, et al. (2003). Oral creatine monohydrate supplementation improves brain performance. Proceedings of the Royal Society B, 270(1529), 2147–2150.
Avgerinos KI, et al. (2018). Effects of creatine supplementation on cognitive function of healthy individuals: A systematic review of randomized controlled trials. Experimental Gerontology, 108, 166–173.
McMorris T, et al. (2007). Creatine supplementation and cognitive performance in elderly individuals. Neuropsychology, Development, and Cognition, 14(5), 517–528.
Candow DG, Chilibeck PD, Forbes SC. (2019). Creatine supplementation and aging musculoskeletal health. Endocrine, 64(1), 49–57.
Forbes SC, Candow DG. (2021). Timing of creatine supplementation and resistance training: A brief review. Journal of Exercise and Nutrition, 4(4).
Hultman E, et al. (1996). Muscle creatine loading in men. Journal of Applied Physiology, 81(1), 232–237.
Kreider RB, et al. (2017). International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. JISSN, 14(1), 18.
Gualano B, et al. (2008). Effects of creatine supplementation on renal function. European Journal of Applied Physiology, 103(1), 33–40.
Antonio J, Ciccone V. (2013). The effects of pre versus post workout supplementation of creatine monohydrate on body composition and strength. JISSN, 10(1), 36.
Lopez RM, et al. (2009). Does creatine supplementation hinder exercise heat tolerance or hydration status? Journal of Athletic Training, 44(2), 215–223.
van der Merwe J, Brooks NE, Myburgh KH. (2009). Three weeks of creatine monohydrate supplementation affects dihydrotestosterone to testosterone ratio. Clinical Journal of Sport Medicine, 19(5), 399–404.
Sakellaris G, et al. (2008). Prevention of complications related to traumatic brain injury in children and adolescents with creatine administration. Journal of Trauma, 61(2), 322–329.