
Blood Flow Restriction Therapy: The Recovery Tool Most Clinics Aren't Using
After surgery, one of the most frustrating realities of recovery is this: your body needs muscle to heal, but you're not allowed to load the tissue enough to actually build it. You're caught in a gap — too fragile for real training, but losing strength every day you're not training.
Blood Flow Restriction therapy (BFR) was developed specifically to close that gap. It's one of the most well-researched innovations in rehabilitation and sports performance over the last two decades, and it's been quietly changing what's possible in post-surgical recovery, injury rehab, and athletic training.
Here's what it is, how it works, and why Ascent Total Performance has integrated it as a core tool in our clinical practice.
1. What Is Blood Flow Restriction Therapy?
BFR therapy involves the application of a specialized pneumatic cuff — similar to a blood pressure cuff — to the upper arm or upper thigh. The cuff is inflated to a precisely calibrated pressure that partially restricts venous blood flow (blood leaving the muscle) while maintaining arterial inflow (blood entering the muscle).
The result: the working muscle is temporarily engorged with blood, creating a metabolic environment that mimics the physiological stress of heavy resistance training — even when the external load is only 20–40% of your normal maximum.
BFR allows you to achieve high-intensity training adaptations at low-intensity loads. That's not a workaround. That's the mechanism — and it's backed by two decades of clinical research.
2. Why It Works: The Physiology Behind the Results
When venous outflow is restricted, metabolites like lactate and hydrogen ions accumulate in the muscle at a much faster rate than normal. This metabolic stress triggers a powerful cascade of physiological responses:
Increased secretion of growth hormone and IGF-1 — key anabolic signals for muscle repair and growth
Activation of fast-twitch (Type II) muscle fibers, which are the primary drivers of strength and power
Upregulation of muscle protein synthesis — the biological process that builds and repairs muscle tissue
Reduction in myostatin — a protein that inhibits muscle growth
The net effect is a training stimulus that approximates the muscle-building response of heavy loading — without the mechanical stress on joints, tendons, or healing tissue. Published research in the Journal of Strength and Conditioning Research, Sports Medicine, and the American Journal of Sports Medicine consistently shows BFR produces significant gains in muscle hypertrophy and strength at loads as low as 20% of 1-rep max.
For patients who can't tolerate heavy loads, that's not a minor advantage. It's the difference between progressing and stalling.
3. Clinical BFR vs. What You See in the Gym
BFR has grown in popularity in fitness settings, and you've probably seen elastic bands or straps used for "occlusion training" on social media. It's worth understanding the difference between that and clinical BFR — because the distinction matters for safety and effectiveness.
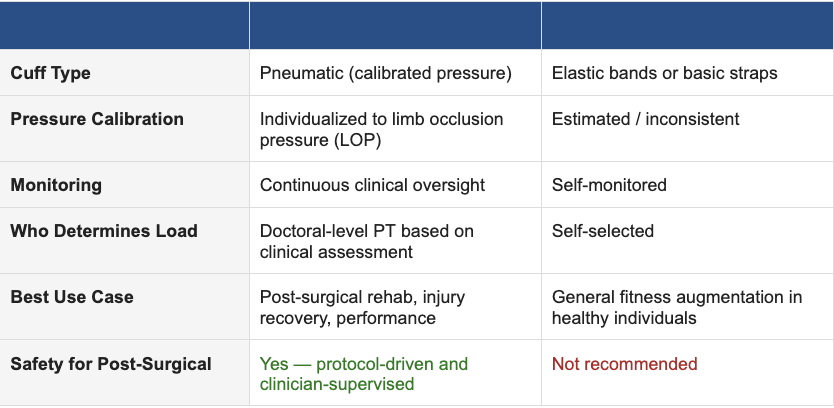
In a clinical BFR protocol, your treating PT measures your Limb Occlusion Pressure (LOP) — the pressure required to fully occlude your artery — and then sets the cuff at a precise percentage of that value (typically 40–80% for the lower extremity, 40–50% for the upper). This individualization is what makes clinical BFR both safe and consistently effective.
Elastic bands can't provide this level of calibration. For post-surgical or injured patients, uncontrolled occlusion pressure is not a risk worth taking.
4. Who Benefits from BFR Therapy?
BFR is a versatile tool. At ATP, we use it across a wide range of clinical presentations and performance contexts:
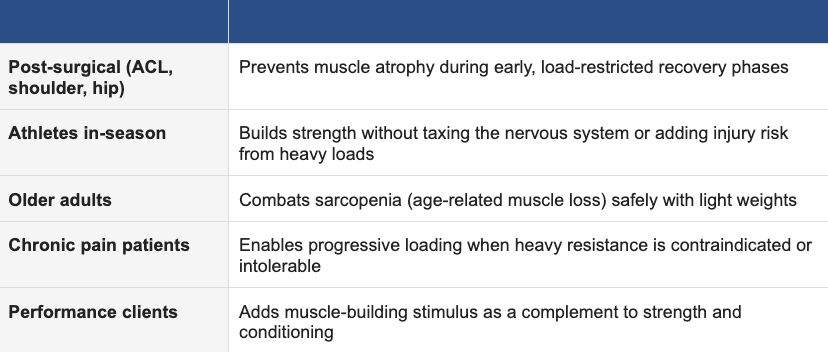
The common thread: anyone who needs to build or maintain muscle but faces a load restriction — whether that's a healing ACL graft, a fragile tendon, an arthritic joint, or the accumulated fatigue of a competitive season.
5. How We Use BFR at Ascent Total Performance
BFR isn't something we bolt onto the end of a session as an add-on. It's a deliberate clinical decision, integrated into a patient's overall treatment program based on their current tissue tolerance, phase of recovery, and performance goals.
In ACL rehabilitation, we begin BFR work in the early post-surgical phase — often weeks one through four — when the graft is too fragile for meaningful quad loading through traditional resistance. BFR lets us begin building the quadriceps immediately, preventing the significant atrophy that derails so many ACL recoveries before they gain momentum.
For post-surgical shoulder patients, BFR allows rotator cuff and periscapular strength work to begin much earlier than conventional timelines allow. This matters because shoulder function is heavily dependent on the small stabilizing muscles — and waiting for tissue tolerance often means waiting too long.
For performance clients and athletes, BFR acts as a high-efficiency stimulus for muscle development — particularly during in-season periods where volume and fatigue management are priorities.
BFR doesn't replace progressive loading. It extends the window in which productive training can happen — so that when you're ready to load heavy again, you're starting from a better foundation.
6. What Does a BFR Session Actually Look Like?
If you're imagining something extreme or uncomfortable, it's worth resetting that expectation. Most patients describe the sensation as a moderate muscle pump — similar to what you feel near the end of a high-rep set. There is a degree of discomfort, but it's muscular, not painful, and it resolves quickly.
A typical BFR protocol looks like this:
Cuff applied to the upper arm or upper thigh and inflated to individualized pressure
Exercise performed at low external load — bodyweight movements, light resistance bands, or light dumbbells
High repetition schemes (typically 30–15–15–15) with short rest intervals (30–45 seconds between sets)
Session duration: 15–20 minutes of BFR work, integrated into a broader PT session
Your DPT monitors your response throughout — watching for appropriate muscle fatigue, checking for skin changes, and adjusting the protocol as needed. Nothing about BFR is left to chance in a clinical setting.
Most patients are surprised by two things: how manageable the experience is, and how significant the fatigue feels relative to the weight they're using. That's the mechanism working exactly as intended.
The Bottom Line
Blood Flow Restriction therapy represents one of the most meaningful advances in rehabilitation and performance training in the last two decades. The research is strong. The clinical outcomes are real. And the patients who have access to it — properly applied by a skilled clinician — recover faster, maintain more strength, and return to their lives and sport with a better foundation.
Most clinics don't offer it. We do — and we've integrated it as a standard part of how we approach recovery for the right patients. If you're dealing with a post-surgical timeline, a load-restricted condition, or you're an athlete looking to optimize your training, BFR may be exactly what's missing from your program.
📅 Want to know if BFR is right for your recovery or training? Request your appointment at achieveatp.com — no referral needed.