
Your MRI Found Something. But Is It Actually Causing Your Pain?
Diagnostic imaging is one of the great achievements of modern medicine. From the first X-ray in 1895 to today's high-resolution MRI, our ability to see inside the human body without a scalpel has transformed how we diagnose fractures, identify tumors, guide surgical instruments, and rule out the serious pathologies that require urgent medical attention. In the right context, imaging is indispensable.
But there's a problem — and it shows up every day in physical therapy clinics across the country. Patients arrive holding an imaging report full of alarming-sounding phrases: "degenerative disc disease," "disc bulge at L4-L5," "grade II labral tear," "facet degeneration," "rotator cuff tendinopathy." Their previous provider pointed to these findings and said: that's what's causing your pain.
Except that's often not what the research supports. The interpretation of imaging findings — not the imaging itself — is where things frequently go wrong.
1. Imaging Provides Data. It Doesn't Always Provide Answers.
An MRI or X-ray is extraordinarily good at showing structure. What it cannot tell you, on its own, is whether a given structural finding is actually responsible for your symptoms. That requires clinical reasoning — a thorough physical examination, a detailed history, an assessment of how you move and what provokes your pain — that no scan can replace.
The critical question researchers use to test whether a structural finding is clinically meaningful is this: how common is this finding in people who have no pain at all? If a "disc bulge" shows up at the same rate in asymptomatic people as it does in people reporting back pain, then the disc bulge is not a reliable explanation for the pain. It may be coincidental. It may be incidental. It may simply be a normal feature of an aging body.
A finding on an image is not a diagnosis. It's data — and data requires interpretation. The question is never just "what does the scan show?" It's "does what the scan shows explain what the patient is experiencing?"
2. What Scans Show in People Who Feel Fine
A landmark systematic review by Brinjikji et al., published in the American Journal of Neuroradiology, analyzed imaging data from over 3,100 asymptomatic individuals — people with no back pain, no leg symptoms, no complaints whatsoever. What they found should change how you read your next imaging report:
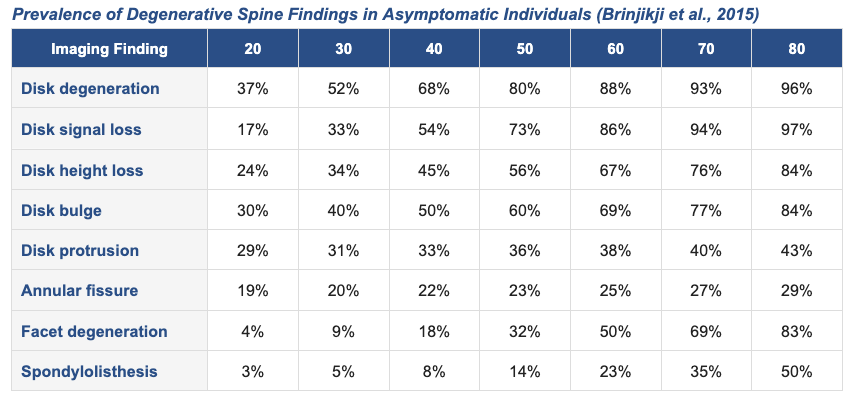
Let that sink in. By age 50, 80% of people with no back pain show disk degeneration on MRI. By age 60, half of all pain-free adults have facet degeneration. A 30-year-old with a "disk bulge" finding has a 40% chance of that being present regardless of whether they ever had back pain.
These are not rare exceptions. These are the expected features of a living, aging musculoskeletal system. Calling them "disease" — and treating them as the source of a patient's pain — is one of the most consequential errors in modern orthopedic and spine care.
3. The Same Pattern Holds for Your Knee and Hip
Spine imaging gets the most attention, but the research on asymptomatic findings extends equally to the knee and hip — two joints where imaging findings are routinely used to explain pain and justify procedures.
A systematic review and meta-analysis published in the British Journal of Sports Medicine (Culvenor et al., 2019) examined knee MRI findings in asymptomatic, uninjured adults. The results were consistent with the spine literature: meniscal abnormalities, cartilage defects, and bone marrow lesions were common across age groups in individuals reporting no knee symptoms.
For the hip, research examining asymptomatic populations has found labral tears and femoroacetabular impingement (FAI) morphology in a substantial proportion of pain-free individuals — including competitive athletes. A tear on a hip MRI arthrogram, in isolation, does not tell you that the tear is generating your symptoms.
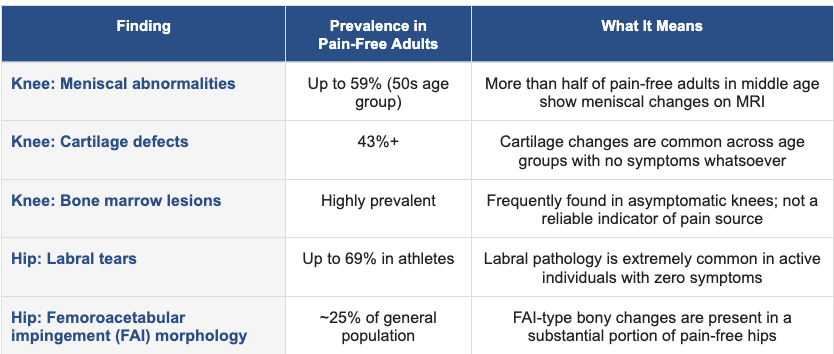
Meniscal tears. Labral tears. Cartilage changes. These are found routinely in people who train hard, live actively, and feel no pain. An image that shows these findings in a person who does have pain is not, by itself, proof of causation.
4. The Usain Bolt Principle
Usain Bolt — the fastest human being ever measured, eight-time Olympic gold medalist, world record holder in the 100m and 200m — has scoliosis. His spine curves significantly to the right, causing a functional leg length discrepancy that biomechanics researchers have studied extensively. By the logic of imaging-driven diagnosis, Bolt should be limited. He should have pain. He certainly shouldn't be running 9.58 seconds for 100 meters.
He did it anyway. Repeatedly. At the highest level of human performance the sport has ever seen.
Bolt's scoliosis is one of the most visible examples of a principle that plays out in clinics every day: structural findings and functional capacity are not the same thing. A spine that looks asymmetrical on an image can belong to the fastest man alive. A meniscus with a degenerative signal can be attached to a knee that runs marathons without a problem.
The inverse is also true — and this is where the real clinical harm happens. A patient receives a report with language like "moderate degenerative disc disease" or "significant facet arthropathy." They are told this is why they hurt. They become afraid to move. They stop exercising. They protect the "damaged" area. And because movement is one of the most effective tools for musculoskeletal pain, the avoidance itself becomes a driver of ongoing symptoms.
Researchers call this the nocebo effect — harm caused not by a treatment but by a belief, often instilled by the language a provider uses to describe a finding. Telling a patient they have a "crumbling disc" or a "torn" structure activates fear, changes movement patterns, and can worsen outcomes independent of any physical intervention. Words on an imaging report carry real clinical consequences.
5. If the Scan Doesn't Explain It, What Does?
Pain is complex. It is influenced by tissue condition, yes — but also by movement patterns, load tolerance, nervous system sensitization, sleep, stress, psychological context, and history. A thorough clinical evaluation explores all of these. It asks: what movements provoke or relieve your symptoms? How did this start, and what has changed? What are you avoiding, and what does that avoidance cost you? What does your body do under load?
These questions cannot be answered by a scan. They require time, clinical skill, and a provider willing to look past the report and actually assess the person in front of them.
At Ascent Total Performance, we treat you — not your imaging. Your scan may be part of the picture, and in cases where it identifies something that changes our approach, we use it accordingly. But a structural finding is never, on its own, the end of the conversation. It's the beginning of a better one.
We assess how you actually move — not just what your anatomy looks like at rest
We identify what is actually provoked by load, position, and movement pattern
We distinguish between structural findings that are clinically relevant and those that are incidental
We build a plan based on what your body can do and what it needs — not on the language in a report
The Bottom Line
Imaging is a tool. Like any tool, its value depends entirely on how it's used and interpreted. A disc bulge is not a death sentence. Facet degeneration is not an explanation for your pain by default. A labral tear in an asymptomatic athlete is not the same clinical entity as a labral tear in a patient who can't sit without pain.
If you've received an imaging report and been told that a structural finding is the reason for your symptoms — or been left wondering what any of it means — come in and let us take a real look. We'll help you sort through the jargon, understand what actually matters clinically, and build a plan around what your body needs.
Disclaimer: This content is for educational purposes only and does not constitute medical advice. Always consult with your physician or a licensed healthcare provider before making changes to your treatment plan.
📋 Got an imaging report you'd like us to help make sense of? Request an evaluation at achieveatp.com — no referral required.
REFERENCES
All studies peer-reviewed and indexed. Verify at pubmed.ncbi.nlm.nih.gov.
Brinjikji W, Luetmer PH, Comstock B, et al. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. American Journal of Neuroradiology, 36(4), 811–816. https://www.ajnr.org/content/36/4/811
Culvenor AG, Øiestad BE, Hart HF, Stefanik JJ, Guermazi A, Crossley KM. (2019). Prevalence of knee osteoarthritis features on MRI in asymptomatic uninjured adults: a systematic review and meta-analysis. British Journal of Sports Medicine. https://bjsm.bmj.com/content/early/2019/08/07/bjsports-2018-099257
Frank JM, Harris JD, Erickson BJ, et al. (2015). Prevalence of femoroacetabular impingement imaging findings in asymptomatic volunteers: a systematic review. Arthroscopy, 31(6), 1199–1204. https://pubmed.ncbi.nlm.nih.gov/25636988/
Moseley GL, Butler DS. (2015). Fifteen years of explaining pain: The past, present, and future. Journal of Pain, 16(9), 807–813.
Darlow B, Dowell A, Baxter GD, Mathieson F, Perry M, Dean S. (2013). The enduring impact of what clinicians say to people with low back pain. Annals of Family Medicine, 11(6), 527–534.
O'Sullivan P, Caneiro JP, O'Keeffe M, O'Sullivan K. (2016). Unraveling the complexity of low back pain. Journal of Orthopaedic & Sports Physical Therapy, 46(11), 932–937.